


Charles Henry Gosselin had not yet turned two years old when the probate court of Providence committed him to the county orphanage in 1924. He spent his infancy there in cottage B before being transferred to the State Home and School. At the age of eighteen, he joined the Civilian Conservation Corps and was assigned to Camp G in Moffat County, Colorado, where he worked as a cook, earning $340 in a year’s time.[1]
In October of 1940, Gosselin enlisted in the United States Army. As a member of the 633rd Anti-Aircraft Artillery, Automatic Weapons Battalion, Battery C, he served in World War II and was honorably discharged on October 31, 1945.
Upon returning to Providence, Gosselin secured employment at Brown & Sharpe, manufacturing tools. After two years on the job, his health had declined so severely that he was forced to retire. A doctor was consulted concerning the 26-year-old’s debilitating illness and provided a diagnosis. Gosselin was suffering from a brain tumor. His physician offered a solution to the malady: a frontal lobotomy.
The lobotomy had been developed in 1935 by Portuguese neurologist Antonio Egas Moniz, who called the procedure a “leucotomy.” The following year, 41-year-old American neurologist Walter Jackson Freeman—who had been studying the brains of deceased psychiatric patients in an unsuccessful attempt to differentiate them from the brains of the mentally well—learned of Moniz’s surgery and believed he had stumbled upon an advancement that would change the world. It appeared to Freeman that altering the frontal lobes of the brain was the cure for mental illness.
Antonio Moniz, who developed the lobotomy in 1935
Freeman modified Moniz’s procedure and, later that year, introduced the frontal lobotomy in America. After receiving anesthesia, a patient’s head was partially shaved. A purple-colored antiseptic and marking die called gentian violet was then applied with a paintbrush, measuring and marking the locations of the skull where a hand-cranked drill would be utilized. On each side of a patient’s head—not far from the hairline—a diamond-shaped hole of about three centimeters was bored through the skull by the sharp, spinning auger. Cuts were then made into each side of the brain, measuring one inch across and two inches deep. A leucotome—a hollow needle with a sharp wire loop at one end—was then inserted. The loop was rotated in a circular motion to sever between six and 12 marble-sized cores of white matter from the prefrontal lobe and the back of the cerebral cortex. Cores were excised at depths of two, three and four centimeters. Unlike Moniz, who removed the material from the head, Freeman allowed the no-longer-functional matter to remain. Once the surgery was completed, the two gaping wounds were washed with saline, and black silk sutures were used to close them. The entire procedure took approximately an hour.
Although Freeman developed the American version of a lobotomy, he was not a surgeon so was unable to perform the operation himself. He teamed up with 32-year-old American neurosurgeon James Winston Watts and carried out what was little more than an experiment on their first human lobotomy patient.[2] Theodore Dudley Hammatt, an employee of the Department of Agriculture in Topeka, Kansas, went to Freeman in September of 1936 to discuss the ailments of his 65-year-old wife, the former Alice Hood, whom he had been married to for 44 years. The couple had brought three children into their family, the first being son Theodore, who succumbed to dysentery at the age of two in 1899. The death changed Alice forever. She and her husband had brought the toddler to Colorado Springs where it was believed the clean air might help him to overcome the malady. When he passed away there, Alice was so overcome with grief that she could not return to Kansas with the body so that it could be buried. She and her husband remained in Colorado while her father conveyed the boy’s remains back home.
Despite welcoming another son and a daughter, Alice could not seem to shake off the anxiety, depression and insomnia that plagued her. When Theodore heard about Freeman’s new procedure, he thought maybe their prayers had been answered. Alice was in a highly agitated state when her husband brought her in for the surgery. She argued profusely that she did not want her head shaved. Freeman restrained the incompliant housewife while promising her that he would not shave her head. This assurance calmed her down somewhat. Once she fell unconscious, he dragged the razor across her scalp.

Dr. Walter Freeman, who introduced and popularized lobotomies in the United States
When Alice awoke, she noticed that her head was shaven but she did not care. Alice did not seem to care about anything. For the first time in a long time, she was calm and content with no sign of sadness, distress, or any emotions at all. Six days later, Theodore reported that Alice was highly agitated, disoriented, and was having problems with language. However, the procedure was considered a success. Alice was no longer depressed and unable to sleep. She died five years later.
The same year that Freeman and Watts operated on Hammett, they performed a lobotomy on 26-year-old Katherine (Leonard) Garver, the wife of farm machine engineer and salesman Lester Wayne Garver. The daughter of a school teacher, Garver had been married for five years and had three children. After the surgery, she kept in touch with Freeman via letter, from the home she shared with her family on Park Avenue in New York. Two years after the procedure he penned her a missive, expressing joy that she was doing well, and no longer suffering with her previous “distressing symptoms.” He asked her, “What about the ‘doubting Thomases’ that advised so strongly against your operation? Have you seen any of them and can you convince any of them that the operation might be of benefit?” Katherine lived until 1993, when she died from complications of Alzheimer’s Disease. Her body was donated to the University of Osteopathic Medicine & Health Sciences in Iowa.
Freeman championed the lobotomy. The side effects did not seem to matter to him, or to most of those caring for a mentally ill family member who sought out the procedure. Lobotomized human beings became dull, lazy, and apathetic. Their intelligence was diminished and their imagination reduced or destroyed. Self-awareness and self-control were often lost, the patient left to linger in a serious vegetative state, or mild stupor, sometimes having become mute. Motivation was wiped away and memories lost. Personalities became infantile. Patients had to relearn how to feed themselves, and became plagued by incontinence. Approximately 75-percent of lobotomy patients underwent significant weight gain after surgery due to extreme increases in appetite. One female patient added more than 100 pounds to her frame within a year after surgery.
Most lobotomized patients who had suffered from hallucinations continued to see and hear things that were not real, but the disorder no longer bothered them. Likewise, those who had physical pain prior to surgery still experienced the pain but simply accepted it. By 1942, Freeman and Watts had performed over 200 lobotomies. They considered 63-percent the patients to have improved, 23-percent to have had no change, and 14-percent to be worse off than they had initially been. For those who showed improvement, approximately 12-percent relapsed within two years.
In 1946, Dr. Freeman was very excited about an innovative procedure he had been working on—the trans-orbital lobotomy. The newly developed surgery was quick, easy, and cost-effective. Because electric shock was used to bring about the same effects as anesthesia, the need and cost of an anesthesiologist was now saved. And because the procedure took only minutes, the use and expense of a hospital room was obliterated. Best of all, according to Freeman, no surgical training was needed to get the job done.
Using a portable electroshock machine, Freeman adjusted the headset on the patient and turned the knobs to send volts of electricity shooting through the brain and rendering the individual unconscious. The doctor would then slide the end of an orbitoclast—a sharp, steel surgical instrument resembling an ice pick—between the eyelid and the eye socket so that it was parallel with the bridge of the nose. Pushed upward at an angle, the end of the instrument would soon bump up against the orbital plate (the thin layer of bone above the eye). Using a surgical hammer, Freeman tapped the instrument until it broke through that portion of the skull. As the blade sunk down about two inches and entered the area of gray matter where nerve pathways ran from the thalamus to the pre-frontal cerebral cortex, the pick would be swung 40 degrees outward toward the edge of the face, then almost back to its original position, severing a considerable portion of nerve pathways so that overly strong emotional impulses from the frontal lobes to the thalamus were unable to pass through. The pick would then be pushed in deeper, swung 20 degrees toward the nose, then 30 degrees toward the outer edge of the face before being lifted up. This was done through both eye sockets. When he noticed that his first patients began to relapse after three or four months, Freeman stopped putting them to sleep before the surgery. Instead, he would carry on conversations with them while he carved inside their heads, taking note of changes in their demeanor as he went on and allowing that to direct his movements with the pick.[3]
Unlike his original lobotomy, this one only took ten minutes to complete. Within twenty minutes, the patient would awake with no shaven head and no memory of what he or she had just been through, although the patient’s reflection in the mirror would display two horribly blackened eyes caused by the breaking of the orbital plate.[4] Blood-stained fluid would often run from the eye, and it was not uncommon for patients to vomit after the procedure.
Freeman performed his first trans-orbital lobotomy on July 17 of 1946. The patient was 29-year-old housewife Sallie Ellen (Hildreth) Ionesco, the wife of watchmaker John Ionesco. Perpetually suicidal and prone to bouts of violent, manic depression, Sallie had spent her teen years as an inmate at the State Home & School for Girls in North Carolina, a juvenile correctional institution. Freeman and Sallie’s family considered the surgery to be a success. Despite her memory being slightly affected, Sallie went on to work as a saleslady at the city news stand in Washington D.C. and later as a chambermaid for the family of farmer Robert Young. She died in 2007.
On February 20, 1947, brain and nerve specialist Dr. Hannibal Hamlin, who resided on Benefit Street in Providence, was appointed neurosurgeon of Memorial Hospital in Pawtucket. Rhode Island’s most outspoken advocate of lobotomy, he gave a lecture on the subject during the annual dinner of the Rhode Island Medical Society, held on May 14th at the Narragansett Hotel.[5] A 1936 graduate of Yale Medical School, Hamlin served as assistant neurosurgeon at Rhode Island Hospital, and Consulting Neurosurgeon at Butler Hospital, The Emma Bradley Home, The Rhode Island State Hospital for Mental Diseases, and several hospitals in Massachusetts.[6] He would go on to act as Associate Surgeon at Miriam Hospital in Providence.[7]
During the 103rd annual meeting of Butler Hospital in Providence, Superintendent Dr. Arthur Ruggles announced that there were plans to include pre-frontal lobotomy in the facility’s therapeutic program. Ruggles described the surgery and noted that it would be applicable only to those with certain forms of severe mental illness.[8]

Postcard of Butler Hospital in Providence, 1907
That same year, Dr. Watts decided that he no longer wanted to work in conjunction with Dr. Freeman. Watts was angry and disgusted at the way in which Freeman had turned a serious and intensive procedure into a routine process. Unaffected by the break, Freeman purchased a van and began traveling cross-country to teach the process of performing trans-orbital lobotomies to any doctor who wanted to learn. His intention was to publicize how inexpensive, easy, and quick this procedure was. His message was that any doctor could do it. One physician who learned the procedure from Freeman began to perform up to 75 trans-orbital lobotomies per day.
Freeman lobotomized patients at each psychiatric hospital he visited during his tour, allowing the staff to witness the ease with which it could be done. In 1948, he stopped in Rhode Island, where the frontal lobotomy was being performed at various hospitals. At the Rhode Island State Hospital for Mental Diseases, he taught doctors his quick, ice pick procedure. That year’s Reports of the Trustees and Superintendent of Butler Hospital noted that the more complex frontal lobotomies were still being carried out as a “continuing project.” The report went on to state that “All cases of frontal lobotomy at this hospital are subjected to extensive testing prior to lobotomy and at periodic intervals after lobotomy. It is hoped that this long-term study will throw more light on the nature of the reaction to frontal lobotomy.”[9]

Postcard of Butler Hospital in Providence, 1910
That was the year that Charles Henry Gosselin’s brain was modified at a hospital in Rhode Island. He was among the nearly 2,000 veterans lobotomized in the United States between 1947 and 1950.[10] In the days following his surgery, Charles began to experience delusions, hallucinations, agitation, and incoherent speech. Unable to care for himself due to psychosis, he was welcomed into the home of 39-year-old Justin Edward McCormick on Arlington Street in Cranston. McCormick and his wife were employed by the state’s welfare services department.
Despite the many horror stories which resulted, Freeman continued to praise the updated and simplified procedure. He announced that the trans-orbital lobotomy did wonders for women who became depressed during menopause. Statistics would later show that approximately sixty percent of all lobotomies in America were performed on females.
Freeman also made appeals to those suffering from any sort of emotional instability, profound grief, or pain and disability that the individual believed to be physical but which might actually be all in their mind. These were just some of the many scenarios in which Freeman felt the lobotomy would be helpful. Individuals suffering from painful terminal illnesses were given the option of being lobotomized. The surgery did not take the pain away, it simply made the patient no longer care about the pain. Likewise, those dealing with intense grief or anxiety could also undergo having the nerves in their brain severed so that they did not have to live the type of life that might eventually lead to drug addiction, depression, or suicide.
Two major reasons for lobotomy, as far as Freeman and those who heralded his procedure were concerned, were financial and familial.[11] It was considered that the mentally ill were a burden on their families, and that anything that might be done to turn a chaotic psychiatric patient into a docile shell of a person was worth it. In addition, psychiatric hospitals were overcrowded and large staffs cost money. The more patients who could have their conditions brought under control so that they could go back home to their families, the better. By 1948, approximately 4,000 Americans had been lobotomized. The next year, Moniz was awarded the Nobel Prize for developing the procedure.
The brain surgery was sought by young and old, rich, and poor. The typical annual income was about $2,600 at that time. A car cost approximately $1,000 and a house set one back approximately $8,000. A lobotomy could be had for less than $250.
Rose Williams, the sister of playwright Tennessee Williams had undergone a lobotomy while in her thirties, to curb her schizophrenia. The botched surgery left her an invalid for life, in the care of various institutions until her death.
Investor and politician Joseph Kennedy had arranged for his 23-year-old daughter Rosemary to undergo the procedure in 1941 in Washington, D.C. Allegedly Rosemary was intellectually delayed as a child. Then, as a young adult, she became argumentative, hostile, and difficult to control. She enjoyed sneaking out with boys and engaging in behavior that would have proven humiliating in a family of high profile men. Dr. Watts performed the surgery on Rosemary, directed by Dr. Freeman. Watts, who believed that Rosemary was not mentally challenged—as her father suggested—but was instead mentally ill, later described the procedure on her, his 66th lobotomy patient. “We went through the top of the head. I think she was awake. She had a mild tranquilizer. I made a surgical incision in the brain through the skull. It was near the front. It was on both sides. We just made a small incision, no more than an inch.” Watts recalled how he asked Rosemary to count and sing while he was cutting into her brain. “We made an estimate on how far to cut based on how she responded,” he explained. The lobotomy rendered the young woman seriously disabled and in need of constant care for the rest of her life. Her parents subsequently deeply regretted having the lobotomy performed on their daughter.[12]
Ways in which to adapt the lobotomy were tackled by doctors across the country, all eager to build on this foundation of innovative advancement. A team of over one-hundred scientists at Columbia University developed a procedure called the topectomy, in which two sections of the frontal cortex—each about the size of a matchbook—were removed in order to suppress anxiety, aggression and the symptoms of Obsessive Compulsive Disorder. It was not suitable for patients with senile dementia or advanced schizophrenia. It caused less severe personality changes than that of Freeman’s lobotomy, but carried over a one-in-ten percent chance of inducing seizures.[13]

Recent photograph by the author of Butler Hospital
During 1949 and 1950, with Dr. Hamlin on the visiting staff of the Rhode Island State Hospital for Mental Diseases, a research project concerning the psychiatric, psychological, and social studies of twenty patients who had been lobotomized between 1947 and 1949 took place. Another later study concerned those lobotomized between 1949 and 1950. Butler Hospital had its own initiative project happening, described as a careful pre and post research project on operative psychological studies and prolonged follow-up of lobotomized patients.[14]
After collaborating with Freeman, Hamlin authored several papers, including “Frontal Lobotomy: Neuroanatomical Observations,” which appeared in the Journal of Neuropathy and Experimental Neurology in July of 1950.[15] That was the month Gosselin’s health began declining so severely that he had to be admitted to the Rhode Island State Hospital for Mental Diseases. At 10:50 on the morning of August 14, he passed away. The 28-year-old was laid to rest in St. Ann’s Cemetery in Cranston.
Experiments in the process of lobotomizing human beings continued. Dr. Hamlin, Dr. Sweet and neuropathologist Paul I. Yakovlev began working on a procedure which entailed the brains of deceased patients who had had frontal lobotomies being serially sectioned after fixation for study purposes. The patients had survived between 32 and 235 days after surgery. Two of the brains were cut open horizontally while the other four were cut in sagittal sections (left and right). In July, Hamlin went on to co-author “Frontal Lobotomy: Neuroanatomical Observations” in the Journal of Neuropathy and Experimental Neurology.[16]
The Boston Psychopathic Hospital announced that over 450 lobotomies had been performed there between 1943 and 1950.[17] Richard Meredith, a 17-year-old boy who had attended Roosevelt High School before being placed at the State School for the Feeble-Minded in Glenwood Hills, Iowa, two years earlier, underwent a lobotomy in 1950. Having loved sports prior to his surgery, the young man continued to play the games he loved and later competed in the Special Olympics. The son of a life insurance salesman, he spent the rest of his life in care facilities, dying in 2013.[18]
By 1951, as many as 51,000 lobotomies had been performed nationwide. That year, 62-year-old Oscar-winning actor Warner Leroy Baxter underwent a trans-orbital lobotomy, in the hopes it would ease the pain of his arthritis. Baxter and his wife, who resided in Beverly Hills, had enjoyed a luxurious life, kept running smoothly by maids, butlers, cooks and groundskeepers After the surgery, the actor was semi-catatonic, with no interest in doing anything. His memory had been destroyed and he was unable to recognize anyone he knew. Worst of all, he began suffering violent convulsions. He passed away in May, only a few months after the procedure, from pneumonia.
While most physicians continued to champion Freeman’s conception despite the drawbacks, others had begun seeking alternative methods of controlling the brains of psychiatric patients. In 1951, Dr. Hamlin teamed up with 36-year-old Dr. Jose Delgado, the pioneer of electrical brain stimulation. A professor of neurophysiology at Yale, Delgado developed methods that allowed him the ability to induce changes in emotion and behavior in animals via electrical stimulation of the brain. The two men worked on their experiment at a now-closed mental health facility in Rhode Island. Selecting 25 patients—the majority of them afflicted with schizophrenia or epilepsy—upon whom treatments for their conditions had not worked, Delgado implanted electrodes in their brains to stimulate the motor cortex. Delgado believed the implants would let doctors know which patients would respond well to a lobotomy.[19]
Delgado had experimented on monkeys before moving on to humans. During a peer interview, he described those experiments:
“I continued on monkeys for seven or eight years. I was able to induce yawning, multiple behaviors, and pupillary dilation so then I decided if it works in monkeys, why not implant electrodes in humans? Now we are in 1952, Providence, Rhode Island where in collaboration with Dr. Hannibal Hamlin, a surgeon, we began implanting electrodes in schizophrenic patients.”
Delgado described how little holes were made in the brain in order to insert the electrodes in the frontal lobe, the thalamus, and the rostral area. “When did you do it for the first time?” he was asked. “In Providence, Rhode Island. In 1952,” he answered, noting that the first patient was schizophrenic and that he went on to implant electrodes into the heads of 35 or 40 patients.[20]
Dr. Delgado later recalled, “In the early 1950s, a patient in a state mental hospital approached Dr. Hannibal Hamlin and me, requesting help. She was an attractive 24-year-old woman of average intelligence and education who had a long record of arrests and disorderly conduct. She had been repeatedly involved in bar brawls in which she incited men to fight over her, and had spent most of the preceding few years either in jail or in mental institutions. The patient expressed a strong desire as well as an inability to alter her conduct and, because psychiatric treatment had failed, she and her mother urgently requested that some kind of brain surgery be performed in order to control her disreputable, impulsive behavior. They asked specifically that electrodes be implanted to orient possible electrocoagulation of a limited cerebral area, and if that was not possible, they wanted a lobotomy.”[21]
Other doctors were also beginning to seek a means of avoiding unsuccessful lobotomies. Experiments were being done with procaine hydrochloride—an anesthetic which blocks sodium channels and paralyzes sensory nerve fibers in order to numb areas of the body.[22] Considered a “trial lobotomy,” procaine hydrochloride was injected through a hole made in the skull, into the brain. Four cubic centimeters of two-percent procaine was injected very slowly and the patient was observed following the procedure. If the symptoms of mental illness declined, it was decided that a lobotomy would be beneficial.[23]

Rosemary Kennedy, daughter of Joseph and Rose Kennedy, and sister of President John F. Kenney (John F. Kennedy Library)
During the summer of 1952, Dr. Freeman traveled to the mid-Atlantic to begin his West Virginia Lobotomy Project. His trans-orbital lobotomy was conducted on 228 psychiatric hospital patients within just twelve days. Quickly and efficiently, Freeman introduced a series of three electric shocks into the brains of each patient—in order to sink them into a five or ten-minute coma—before inserting his pick under each eyelid and plunging it about two inches deep to sever the fibers there. Four of the patients died from the procedure. The later results of the experiment showed that 126 patients had either no improvement or only partial improvement.
Freeman’s project continued with nearly 400 more patients collected within West Virginia’s four psychiatric hospitals. Like most of the others in the project, the patients became tranquil and cooperative after the surgery. This state of being lasted for about two weeks. For the next six weeks to six months, irritability and defiance took over. Some would later return to their post-operative nearly-vegetative state while others would revert back to their pre-surgical behaviors and conditions.[24]
In 1953, 27-year-old Henry Gustave Molaison had his hippocampus removed from deep within the brain’s temporal lobe during a lobotomy. It was hoped the procedure would curb his epilepsy. Following the surgery, he could no longer form memories. His family cared for him until he was moved into a nursing home during the 1970s. He died there in 2008 of respiratory failure. His brain was preserved for study.
The families of mentally and physically ill individuals continued seeking out doctors to attempt a quick fix upon the brain of their loved ones. Moniz’s frontal lobotomy was still largely considered an advantageous operation within the medical community, while Freeman’s trans-orbital lobotomy began to fall out of favor.[25] In July 1953, Freeman was removed from his position as Consultant in Neurology at St. Elizabeth’s Hospital in Washington, D.C. The superintendent of the facility, Dr. Winfred Overholster, decided that he felt the trans-orbital lobotomy was “drastic and mutilating.”
At the end of the following year, the Lobotomy Program in Rhode Island recorded five pre-frontal lobotomies performed by the State’s neurosurgical consultant.[26] Dr. Hamlin, who served as President of the New England Neurosurgical Society from 1953 to 1954, continued to offer his services at Rhode Island’s State Hospital of Mental Diseases, Rhode Island Hospital, and Miriam Hospital. Although he still saw the value in lobotomy, there were now doctors who wanted no part of it and that position widened over the next few years.
Dr. Percival Bailey, director of the Illinois State Psychiatric Institute, went on record in 1956 to announce that he was personally “appalled” by the use of lobotomy. Bailey explained that the only success which came from lobotomy was that of making the afflicted easier for their family to care for. Lobotomy, he argued, was merely a substitute for allocating money to psychiatric hospitals so that they could employ larger staff.[27]
The case of Margaret (Willix) Dugan versus the United States was heard in 1956, two years after her husband was killed by a lobotomy patient. Robert Aloysius Dugan was a 65-year-old veteran afflicted with tuberculosis, frailty, and poor mental health. During the summer of 1954, he had been a patient at St. Elizabeth’s Hospital, one of the largest psychiatric hospitals in the country, and the facility that had recently dropped Dr. Freeman from its staff. On the morning of July 13, 1954, Robert Dugan was in the lavatory of his ward with two other patients. One of the patients, a man named Broddgarrd, had undergone a lobotomy in the hopes of curbing his violent behavior. The operation had been deemed a success because, since the procedure, he had been peaceful and obedient and done nothing worse than kick another inmate in the shin. But that morning, he gave Dugan a fatal blow to the chest. The single witness to the attack later stated that it was totally unprovoked. Dugan died as the result of fractured ribs and a punctured lung. Mrs. Dugan was unsuccessful in her fight against what she believed to be negligence, and the case was dismissed.
Some doctors got creative with the idea of lobotomy and tweaked it in unique ways. Around 1957, a neurosurgeon named Dr. L. M. Weinberger invented a type of lobotomy that involved burning areas of the brain with boiling water. As a cure for unendurable pain, needle-sized holes were drilled into the skull and boiling salt water was injected. The water was heated to 100 degrees and injected in five cubic centimeter doses until between 15 to 30 cubic centimeter doses had been introduced into each lobe. Within just fifteen minutes, the water would destroy certain frontal lobe tissues. Weinberger conducted his experiments on dogs before taking on human patients.[28]
Vintage postcard of Exeter School for the Feeble-Minded (later known as Ladd School)
Various “cures” for mental illness, including those worked upon the foundation of lobotomy, were introduced by doctors hoping to make a name for themselves by changing the face of medicine. Mental illness proved to be a clever disease—difficult to understand even by the most educated of health professionals. Many agreed that the root cause lie in the frontal cortex of the brain and that anxiety and depression was caused when worry became too heavy, interfering with the flow of messages through the brain and causing the frontal cortex to become swamped. The result was believed to be a cerebral traffic jam that impacted mental health.
In 1960, Dr. Freeman lobotomized 12-year-old Howard Dully, who had a history of being defiant and disobedient. Over the course of his medical career, he would perform approximately 4,000 trans-orbital lobotomies, without any sort of surgical training. Visiting psychiatric hospitals in 23 states over the span of four decades, nearly 500 patients died during or directly following lobotomy, most from the effects of cerebral hemorrhage. One patient died while Freeman stopped mid-procedure to pose for a photograph.[29]
Freeman’s final lobotomy occurred in 1967. Helen Margaret Mortenson was a 50-year-old Minnesota native. Employed as a stenographer who would later work as a secretary for a building and engineering company, she had come to Freeman for her first lobotomy in 1946. Feeling as if the successful results were wearing off in 1956, she had scheduled a second lobotomy with him. Now she was back for a third. There at Herrick Hospital in Berkeley, California, Freeman accidentally tore a blood vessel in her brain. She died of cerebral hemorrhage on February 24, 1967, three days after the surgery. Dr. Freeman, then about 72 years old, was banned from performing any further surgical procedures.[30]
Freeman’s case files are virtual collages of what human beings have done to each other—in the name of medicine, of technological advancement, of award-winning developments. They are proof that “the greater good” pays no attention to the individual. The files include before and after photographs. Most patients are sullen-looking before the procedure and smiling after. Many have partially shaved heads. Freeman noted on one woman’s file that she now “giggles a lot.” Another set of photos shows a woman who had been depressed for four years and constantly complained that her eyes hurt. One year later, Freeman recorded that she was “indolent and euphoric and subject to convulsive seizures, but she made no complaint.”[31]
Among Freeman’s lobotomy patients were at least nineteen children, the youngest being four years of age. A set of photos concerning a six-year-old patient contain the notation that the girl received a lobotomy on August 24, 1944, due to destructive behavior. When the procedure was deemed ineffective, she underwent a second lobotomy on April 26, 1945. Docile for eight months, she eventually resumed smashing her toys. She stares out blankly from her photographs. The majority of doctors who performed lobotomies conducted them upon children as well as adults. Dr. Hamlin performed a lobotomy on a 12-year-old boy at Boston State Hospital on December 7, 1964.[32]
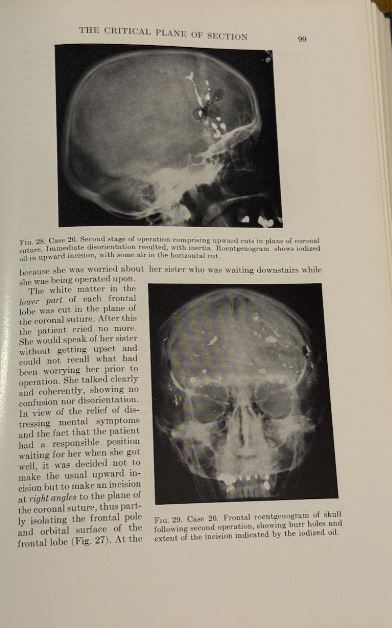
Images from Dr. Walter Freeman’s book, Psychosurgery: Intelligence, Emotion and Social Behavior Following Prefrontal Lobotomy
During the 1970s, lobotomies fell out of favor as psychiatric medications were developed. The lobotomy, as a successful neurosurgical treatment for psychiatric disorders and neurological issues became discredited by the medical community at large. Ken Kesey’s novel, One Flew Over The Cuckoo’s Nest (1962), and the film it inspired by the same name (1975) helped create in the population at large a deep skepticism about the use of lobotomies and electroshock therapy. In the film “The Lobotomist,” produced by Barak Goodman and John Maggio in 2008, the procedure is referred to as “One of the most barbaric mistakes in modern medicine.”
Notes:
[1] “Cranston Man’s Story Has Unknown Beginning,” By Kelly J. Sullivan, Cranston Herald, March 2024.
[2] Michael Robertson and Gary Walter, Ethics and Mental Health: The Patient, Profession and Community,” (Milton Park, United Kingdom: Taylor & Francis, 2014).
[3] “Lobotomy: Intentions, Procedures, Effects,” 2021, Indiana Medical History Museum website, https://www.imhm.org/page-1854827
[4] “Simplified Surgical Technique For Aiding Mentally Ill,” by Thomas R. Henry, The Evening Star (Washington, D.C.), May 20, 1948.
[5] “Doctors to Witness Memorial Award,” The Pawtucket Times, May 14, 1947
[6] “Hospital Names Neurosurgeon,” ibid., February 20, 1947.
[7] The Jewish Herald (Rhode Island), February 4, 1949.
[8] “Butler Hospital Shows Deficit,” The Pawtucket Times, January 22, 1947.
[9] Reports of the Trustees and Superintendent of Butler Hospital, 1948.
[10] Michael Phillips, “Thousands of Military Veterans Were Lobotomized After World War II, The Wall Street Journal, December, 13, 2013.
[11] Dr. James W. Barton, “Operation To Relieve Intense Pain,” The Poplar Standard, Montana August, 26, 1949.
[12] Quoted in Ronald Kessler, The Sins of the Father: Joseph P. Kennedy and the Dynasty He Founded,” (New Yrok: Warner Books, 1966)..See also David Nasaw, The Patriarch, The Remarkable Life and Turbulent Times of Joseph P. Kennedy (New York: Penguin Press, 2012).
[13] Dr. Ryan Holland, Dr. David Kopel, Dr. Peter Carmel, and Dr. Charles Prestigiacomo, “Topectomy versus Leucotomy: J. Lawrence Pool’s Contribution to Psychosurgery,” The Journal of Neurosurgery, Vol. 43, Issue 3 (2017).
[14] “Proceedings of the First Research Conference on Psychosurgery,” Public Health Service publication #16 (1951).
[15] “Frontal Lobotomy: Neuroanatomical Observations,” By P.I. Yakovlev, H. Hamlin, and W.H. Sweet, The Journal of Neuropathy and Experimental Neurology, Vol. 9, Issue 3 (July 1950).
[16] “The Yearbook of Neurology, Psychiatry, and Neurosurgery.” (Edited by Roland P. Mackay, Nolan D.C. Lewis, and Percival Bailey, Year Book Publishers, Illinois, 1950).
[17] Milton Greenblatt, Studies in Lobotomy (New York: Grune & Stratton, 1950).
[18] Obituary of Richard Meredith, The Des Moines Register, September 15, 2013.
[19] “Electrical Activity after Stimulation and Electrocoagulation of the Human Frontal Lobe,” The Journal of Biology and Medicine (December 1955).
[20] “An Oral History of Neuropsychopharmacology: Peer Interviews,” American College of Neuropsychopharmacology (2011).
[21] Jay Katz, Experimentation with Human Beings, (Published by The Russell Sage Foundation, New York, 1972).
[22] Dr. James W. Barton, “Operation To Relieve Grief and Pain May Not Be Necessary,” The Sunday Star (Washington, D.C.), August 10, 1952.
[23] Dr. Orville T. Bailey, Dr. Wilfred T. Small, and Dr. Franc D. Ingraham, “Procaine Block of Frontal Lobe White Fibers as a Means of Predicting the Effect of Pre-frontal Lobotomy,” The Journal of Neurosurgery, Vol. 9, Issue 1, 1951.
[24] “Mass Surgery to Help Insane Praised In West Virginia,” The Evening Star (Washington, D.C.), August 24, 1952.
[25] “The Legacy of Patient H.M. for Neuroscience,” The National Library of Medicine, 2009, https://ncbi.nlm.nih.gov
[26] Rhode Island Department of Social Welfare Reports, 1953, Rhode Island Department of State Archives.
[27] Robert Goldenstein, “Expert Blasts Treatment for Mental Ills,” The Key West Citizen (Florida), May 7, 1956.
[28] Thomas R. Henry, “Boiling Water Injected Into Brain To Ease Pain,” The Evening Star (Washington, D.C.), November 9, 1957.
[29] “My Lobotomy: Howard Dully’s Journey,” website, November 16, 2005, https://www.npr.org/2005/11/16/5014080/my-lobotomy-howard-dullys-journey
[30] “Lobotomy: Intentions, Procedures, Effects,” Indiana Medical History Museum, website, 2021, https://www.imhm.org/page-1854827
[31] Carla Garnett, “When Faces Made the Case for Lobotomy,” National Institute of Heath Record, November 1, 2019.
[32] Vintage Everyday, website, 2018, https://www.vintag.es/2018/12/lobotomy-before-and-after.html
[In the preparation of this article, various birth, death, and marriage records were utilized, along with military records, state directories, census records. and cemetery records.]
The Author
You Might Also Like























{kind=link}